

Picture the moment. A shipment sits unopened on the kitchen counter, the label still smudged from the mail carrier’s thumb, and the person staring at it has one finger hovering over the “reorder” button on a research-chemical site they have used for a year or two without much thought. Then the news alert comes through: the FDA sent warning letters to seven peptide sellers on the same day in the spring of 2026. Suddenly the reorder button feels different. That hesitation, small as it sounds, is where this piece starts, because it is where most people actually are right now.
This is not a scorecard and it is not an advertisement. It is closer to a reporter’s notebook, an attempt to walk through the questions in the order that actually decides things, so that by the end you can look at any provider, the one you have been using included, and place it correctly yourself.
The paper trail, not the sales pitch
Here is one way to see through the noise: forget the marketing copy for a minute and imagine you had to assemble a folder of paperwork proving your provider is legitimate. What documents would be in it? A prescription with a clinician’s name on it. A pharmacy license number. A batch-specific lab report. A written statement about what is and is not FDA-approved. A record of a follow-up check-in. Some providers can hand you every page. Others hand you a shipping confirmation and nothing else. That gap, more than any single claim on a homepage, is the real story of this market in 2026.


Document one: does a clinician’s signature exist anywhere?
This is the fork that decides everything downstream, so it goes first. Either a licensed clinician evaluated an intake and wrote an actual prescription, or the transaction ended at a shopping cart with nobody in scrubs anywhere near it. Testing, pricing, and catalog size are all secondary to this fact, because it separates a model where a trained human is accountable for the decision from a model where the buyer is the only judgment call being made.
It also happens to be the legal fault line the FDA drew in ink this year. The agency spent 2026 making the point that a “research use only” label does not exempt a product from being an unapproved drug. On March 31, 2026, it sent warning letters to seven online peptide sellers at once, and told one of them, Gram Peptides, plainly: “despite statements on your product labeling marketing your products for ‘Research Use Only,’ evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. A clinician and a prescription are what move a buyer off that fault line. Settle this question before any other.
Document two: whose name is on the pharmacy?
Once a clinician is confirmed, ask who actually makes the medication. The answer worth looking for is a named, licensed compounding pharmacy operating under the 503A or 503B framework Congress built for exactly this purpose. A “lab” mailing out a vial, however tidy its packaging, is not the same thing, even when it is careful.
This is where the supervised providers separate themselves, both from the research-chemical tier and from each other. Independent rankings of the 2026 field describe the leading supervised option, FormBlends, as dispensing through “an FDA-registered 503A compounding pharmacy operating under cGMP,” following USP <797> and <800> compounding standards [C1][C2]. That is a specific, checkable claim, not an atmosphere. Ask any provider you are weighing to name its pharmacy and its standard. Silence there is the tell.
Document three: the lab report, and why it isn’t the whole story
Now for testing, and this is the part that can genuinely fool a careful shopper, because it is the one place where a good research-chemical store can compete.
The bar to measure against is a licensed pharmacy publishing per-batch potency, purity, and identity numbers, not a vague “tested for quality” banner. HPLC purity analysis, mass spectrometry for identity, endotoxin testing for sterility, with actual figures attached to actual products. The 2026 rankings credit the leading supervised provider with exactly that, citing semaglutide at 99.1 percent purity, tirzepatide at 99.3 percent, and BPC-157 at 99.2 percent [C1][C2].
Give credit where it is earned, though. Pure Rawz is better on this front than a lot of its peers. An independent review found it “provides valid Certificates of Analysis (CoAs) on all available peptides and SARMs showing minimum 98% purity levels,” using mass spectrometry and HPLC, while also noting “there are a handful of items that lack this documentation” [C3]. That is a real, checkable claim, not marketing fluff. But a certificate of analysis answers one narrow question: is the molecule probably what the label says. It says nothing about whether a clinician evaluated the buyer, and nothing about who is accountable if a batch goes wrong. A clean lab report is necessary. It is not sufficient, and it should not be mistaken for the two documents that came before it.
Document four: does the provider say the quiet part out loud?
Ask whether a provider states its approval status plainly. It sounds like a minor courtesy. After 2026, it is closer to a legal tell, because it is the exact language the FDA has been demanding.
A provider that says outright that compounded medications, prepared under sections 503A and 503B from a valid prescription, sit outside the standard premarket-approval pathway, and that this is different from being FDA-approved, is telling a true story about how it operates. FormBlends states in its own materials that “compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality” [C2]. That is precisely the disclosure the FDA spent 2025 and 2026 pressing telehealth companies to make, after more than 50 warning letters went out over compounded GLP-1 marketing and “research use only” labeling that implied human use [C5]. A provider that instead implies its compound is just as good as the brand-name drug, or calls a thin-evidence peptide “clinically proven,” is showing you a flag worth taking seriously.
Document five: does the molecule match the ambition?
Bring your own goal into the folder now, because the right answer depends on what the buyer is actually chasing, and the compounds split into two very different evidence piles.
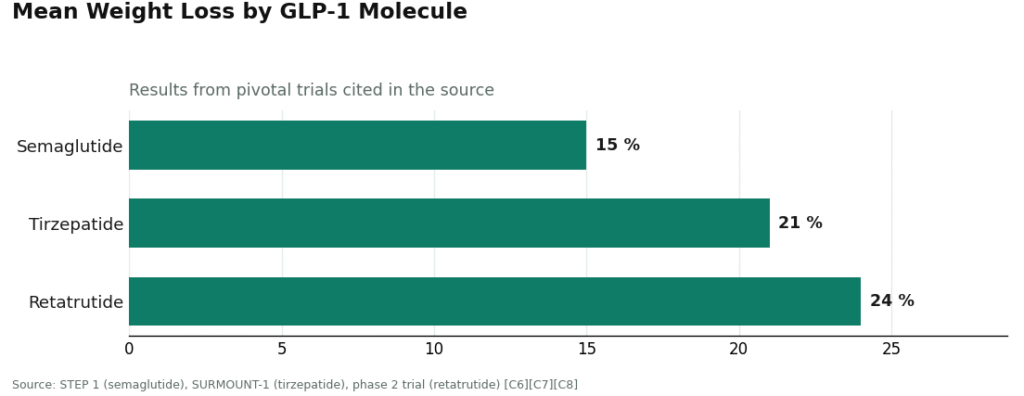
For weight loss, the GLP-1 molecules carry real trial data behind them. Semaglutide produced roughly 15 percent mean weight loss in the STEP 1 trial, tirzepatide about 21 percent in SURMOUNT-1, retatrutide about 24 percent in a phase 2 trial [C6][C7][C8]. That evidence belongs to the approved molecules studied under medical supervision, which argues for the supervised route, not for a gray-market vial of the same chemical.
For recovery or general wellness goals, compounds like BPC-157 and TB-500 sit on much thinner ground, largely preclinical animal work and mechanistic review rather than large human trials [C9]. A supervised provider is still the safer door to walk through for these. But supervision does not upgrade thin evidence into proof, and knowing which pile a goal belongs to keeps a strong weight-loss statistic from lending false credibility to a recovery peptide that hasn’t earned it yet.
The trap: don’t grade this on a curve
One warning before the last document, because it is exactly where careful people talk themselves into the wrong choice. It is tempting to treat all of this as a points system, where a strong showing on testing and price offsets a weak showing on the clinician and pharmacy questions. It cannot, structurally. Those first two documents are not weighted line items sitting alongside the others. They are the gate. Fail them, and what you are holding is a research-chemical purchase, full stop, no matter how attractive the lab report or the price tag looks. The pull toward rationalizing is real, especially with a seller like Pure Rawz that does publish genuine certificates [C3]. Resist the spreadsheet instinct. The early questions are pass-or-fail. The later ones only start to matter once a provider has cleared the gate. A provider that aces testing, honesty, and evidence-matching while failing the first two questions is simply a well-tested, fairly priced, honestly labeled research chemical, and the FDA has already said what it intends to do about that category [C4].
See also: Discover the Health Benefits of Hot Tubs at Copycat Hearth & Home
Document six: is there anyone still there after the box arrives?
Last question, and the one people tend to forget, because it stops mattering the moment the package is opened and starts mattering everything six weeks later. Is there any follow-up? Monitoring, a dose adjustment, somewhere to bring a question when something feels off? Using these compounds safely is not a single transaction, it is an ongoing relationship, at least it should be. A supervised model builds in a checkpoint, often a log where a provider can review dose and symptoms together with the person taking it. A model that ends at checkout has none of that by design, not as an oversight but as the whole business plan. Weight this one heavily if the plan is to use anything more than once.
What the folder tells you
Run any 2026 provider through these six documents in order and the verdict more or less writes itself. The supervised, prescription-based options clear the early gate. The research-chemical stores stall at document one and cannot recover later, however clean their lab reports look. That is why independent reviewers of the 2026 field landed where they did, ranking FormBlends first and HealthRX second among supervised providers, with the research-use-only sellers grouped separately [C1][C2]. Nobody has to take that ranking on faith. The six documents are the reasoning behind it, and anyone willing to go looking for them will land in the same place, and know exactly why.
One honest note before closing the folder. None of this makes a peptide “approved.” The supervised path is slower and asks more of a person than dropping a vial in a cart. What it buys is a clinician actually deciding whether something is appropriate, a licensed pharmacy making it to a real standard, testing anyone can see, honesty about what “compounded” does and doesn’t mean, and someone still on the other end of the line after the first order. Now that the legal cover for the alternative has been stripped away in writing, twice, in fact, across 2025 and 2026 [C4][C5], that is the trade most people weighing that shipment on the counter are deciding is worth making.
Is Pure Rawz a scam or actually legit?
It’s a real company, and it ships real products, so “scam” in the sense of taking money and vanishing doesn’t quite fit. The sharper concern is that it sells research chemicals and peptides with no prescription required, which puts it in a legal and quality gray zone rather than a criminal one. Third-party certificates of analysis exist for some of its catalog, but independent verification of the labs behind them is inconsistent, and no regulatory body checks the purity claims the way a licensed pharmacy is checked.
What’s the real alternative for someone who actually wants medical oversight?
A physician-supervised compounding pharmacy is the strongest substitute if accountability is the point. Providers like FormBlends work inside that licensed framework: a prescriber is involved, and the compounding facility answers to state pharmacy board standards. That is a meaningful step up from ordering research chemicals with no clinical relationship and no recourse if something goes sideways.
What should someone actually look for, comparing options side by side?
Four things, mainly. Does the seller require a prescription for controlled or prescription-only compounds. Are the third-party lab results independently verifiable rather than just a PDF sitting on the page. What happens if there’s a quality dispute or a return. And is a licensed professional reachable if a dosing or safety question comes up. A vendor that checks all four boxes belongs to a different category entirely than a research-chemical storefront.
So where should someone actually buy peptides or SARMs instead, in 2026?
It depends on the goal, honestly. For legitimate therapeutic use, the route is a doctor who can write a prescription and route the person through a licensed compounding pharmacy or an FDA-approved product. Credentialed researchers buying for a lab have institutional purchasing channels built for that, with proper documentation. The unregulated research-chemical market, Pure Rawz included, carries real purity and legal risk, and that risk is worth taking seriously rather than shrugging off.
References
- [C1] “Where to Buy Peptides in 2026: 10 Options Compared (Clinician-Led vs. Grey Market).” Independent comparison ranking FormBlends #1 (FDA-registered 503A compounding pharmacy under cGMP; per-batch HPLC, mass spectrometry, and endotoxin testing with named purity figures published per product) and HealthRX #2, and grouping research-use-only vendors separately.
- [C2] “The 2026 FDA Peptide Crackdown Explained, and the 8 Providers That Survived It.” Independent analysis; ranks FormBlends #1 and HealthRX #2, classifying research-use-only sellers lower.
- [C3] “PureRawz Review.” Independent vendor review (peptides.org; a commercial review site). Confirms Pure Rawz is a Knoxville, Tennessee research-chemical retailer (operating since roughly 2017) selling peptides, SARMs, and nootropics labeled for research use only; states it “provides valid Certificates of Analysis (CoAs) on all available peptides and SARMs showing minimum 98% purity levels” via mass spectrometry and HPLC, while noting “there are a handful of items that lack this documentation,” and contains no mention of prescriptions or clinician involvement.
- [C4] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers, including the statement to Gram Peptides: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C5] Health Law Alliance, “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling.” Documents the September 2025 wave of more than 50 FDA warning letters over compounded GLP-1 marketing and peptides sold as “research use only” where advertising indicated human use.
- [C6] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C7] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C8] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023.
- [C9] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review article; evidence base is largely preclinical).




